In areas where hookworm infection is common (areas with hot and humid climates), also administer antihelminthic treatment from the second trimester:
albendazolePO: 400 mg single dose (ormebendazolePO: 100 mg twice a day for 3 days)
– In areas where malaria is endemic, also administer intermittent preventive antimalarial treatment or curative antimalarial treatment depending on the
results of the screening tests (see below).
Presence of anemia
In the presence of clinical (pale palms, conjunctiva, tongue) or biological anemia (hemoglobin < 11 g/dl in the first and third trimester or < 10.5 g/dl in the second trimester)
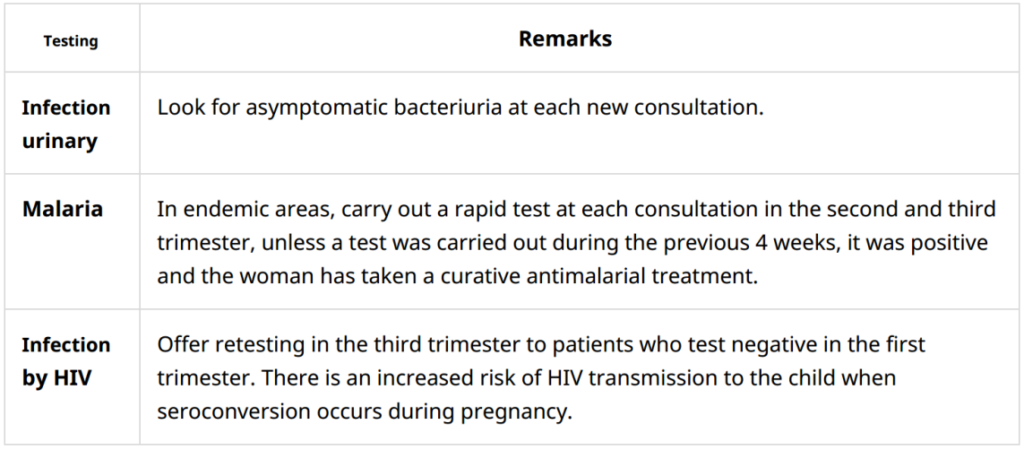
Malaria
In all regions where the transmission of malaria to P.falciparumis moderate to strong,prevention is based on:
– The use of mosquito nets impregnated with insecticide (provide 2 mosquito nets).
– Malaria screening at each prenatal consultation in the second and third trimester:
• If the test is positive, whatever the region and whatever the term of the pregnancy:
Administer a curative antimalarial treatment
After a curative treatment, wait a month to repeat a malaria screening test.
• If the test is negative, Intermittent Preventive Treatment (IPT) is recommended in areas of Africa where transmission of malaria from P.falciparumis moderate to strong.
Start an IPT with sulfadoxine/pyrimethamine(MS)[4]from the start of the second trimester. The aim
is to administer at least 3 doses between the second trimester and delivery with an interval of at least 1 month between each treatment. The number of treatments is not
limited as long as an interval of one month is respected between each treatment. The SP dosage for each treatment is 3 single dose tablets. This treatment reduces the consequences of malaria (maternal anemia, low birth weight). Do not administer this intermittent treatment to HIV-infected women on co-trimoxazole
prophylaxis.
Vitamin and micronutrient deficiency
Calcium
Supplementation is recommended for[6]:
• all pregnant adolescents (under 20);
• all pregnant women whose diet is low in calcium AND who present a high risk of pre-eclampsia (history of pre-eclampsia or eclampsia, twin pregnancy, chronic hypertension).
Start supplementation from the first prenatal visit and continue throughout pregnancy:
calcium carbonate PO: one 1.25 g tablet (equivalent to 500mg of elemental calcium per tablet) 3 times a day
Respect an interval of 2 hours between the administration of calcium and iron salts.
– Vitamin D
Sources of vitamin D are exposure to sunlight and food.
Supplementation is considered if there is a risk of deficiency (low exposure to the sun, diet low in vitamin D): cholecalciferol (vitamin D3) or ergocalciferol (vitamin D2) PO: 100,000 IU single dose at 6 or 7 months of pregnancy
– Iodine
Iodine deficiency during pregnancy exposes you to a risk of abortion,
premature delivery, major mental retardation and weight loss in the child, neonatal and infant death. In areas where iodine deficiency is endemic, iodine supplementation is necessary. Comply with national protocol.
B. Estimation of gestational age and expected date of delivery
Malnutrition
– In case of malnutrition, include the woman in a therapeutic nutritional program. If no nutritional program is in place, provide supplementation:
• BP 190-230 mm: 2 sachets of Plumpy’nut or 3 bars of BP100 per day;
• MUAC < 190 mm: 4 sachets of Plumpy’nut or 7 bars of BP100 per day.
– In the absence of signs of malnutrition but in a situation of food shortage, supplement all pregnant women throughout pregnancy.
– In case of overweight or obesity, provide advice to avoid excessive weight gain during pregnancy.
HIV infection
If positive, start antiretroviral therapy